Pre-exposure prophylaxis (PrEP) is a medication to prevent HIV infection in HIV-negative people. PrEP can stop HIV from taking hold and spreading throughout the body, and when taken daily, oral PrEP is highly effective for preventing HIV from sex or injection drug use. Additionally, expectant mothers who are HIV-negative can take PrEP to prevent infection, and thus prevent mother-to-child transmission (MTCT), during the critical periods of pregnancy and breastfeeding.[1] PrEP and the prevention of MTCT greatly contribute to the UNAIDS “fast-track” targets for prevention, which aims to reduce the number of new HIV infections in 2030 to fewer than 200,000.[2]
Despite scale-up of HIV testing and treatment in Africa, adolescent girls and young women (AGYW), as well as individuals in sero-discordant relationships, have high incidence of HIV. I-TECH supports PrEP delivery at HIV care and treatment clinics for partners of individuals receiving antiretroviral therapy (ART). In addition, I-TECH’s work in PrEP coincides with its efforts to support programs that provide for the physical and mental health of AGYW.
In partnership with the Elizabeth Glaser Pediatric AIDS Foundation, I-TECH faculty Jeff Lane and Aaron Katz prepared the briefs in the sidebar, which outline policy considerations for the scale-up of PrEP for adolescent girls and young women (AGYW) in Kenya, South Africa, and Uganda.
World Health Organization (WHO). WHO expands recommendation on oral pre-exposure prophylaxis of HIV infection (PrEP). Policy Brief. November 2015.
UNAIDS. Understanding Fast-Track: Accelerating Action to End the AIDS Epidemic by 2030. June 2015.
The ZimPAAC consortium collaborates with the Ministry of Health and Child Care (MoHCC) in Zimbabwe to meet the following primary HIV epidemic control objectives:
Diagnose 95% of all persons living with HIV through integrated testing
Ensure 95% of individuals diagnosed with HIV are initiated on antiretroviral therapy (ART), retained in care, and are virally suppressed using differentiated service delivery models
Using a Differentiated care model, a patient-centered model of service delivery designed to meet the diverse needs and expectations of all people living with HIV, ZimPAAC oversees activities such as:
facility and community-based HIV testing;
HIV self-testing, index case testing;
ART initiation; and
ART delivery through multi-month refills for stable patients, Family ART Refill Groups, and Community ART Refill Groups (CARGs). CARGs benefit group members—through decreasing health center visits, offering peer support, and allowing clients to take responsibility for their health—and staff, by decreasing workload and allowing greater time for patient care.
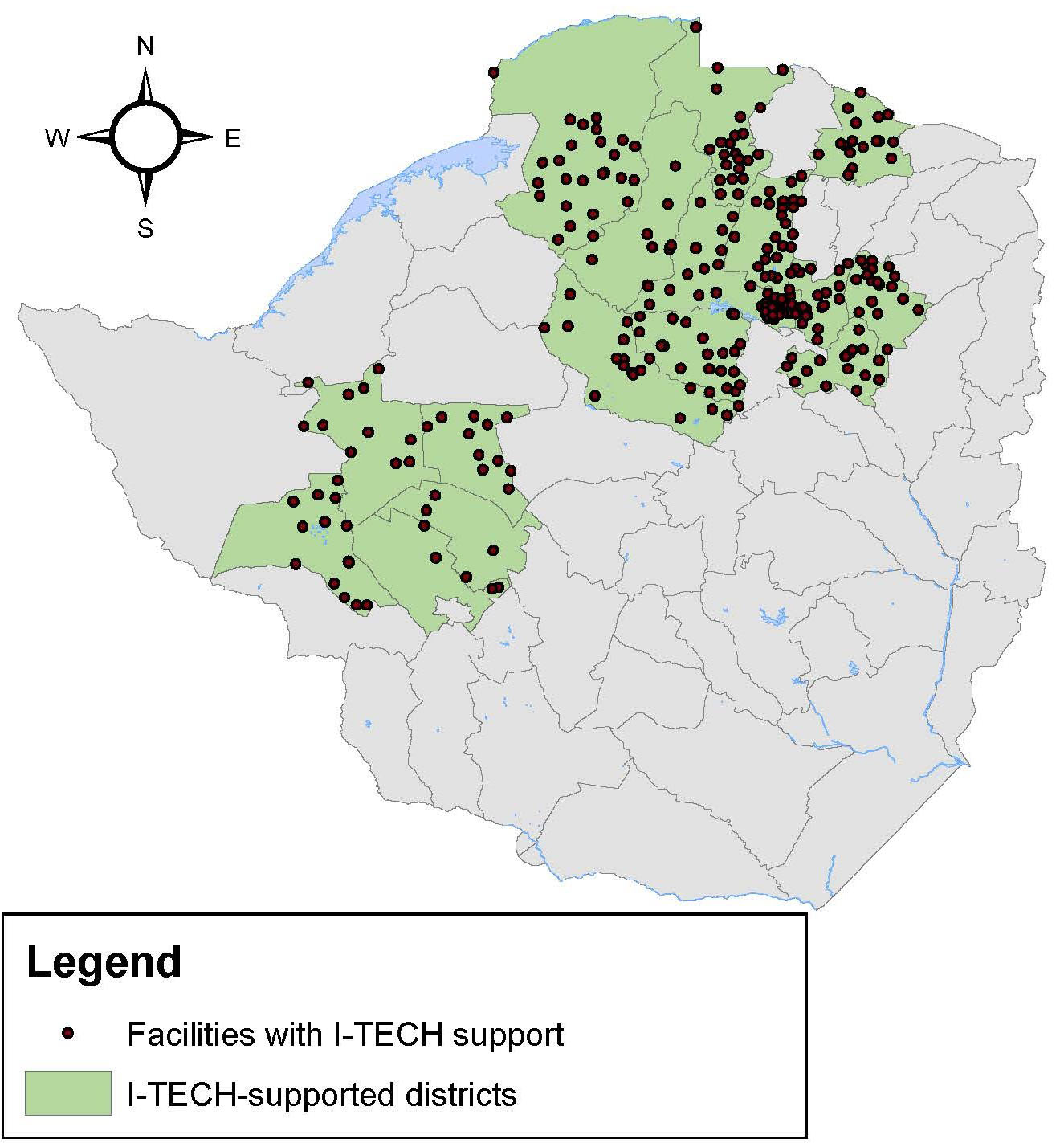
A map of I-TECH’s Care and Treatment Sites and Districts in Zimbabwe.
In addition to differentiated service delivery, ZimPAAC conducts site-level mentoring at health facilities to strengthen health service delivery towards the “95-95-95” UNAIDS targets by improving patient linkages between HIV testing, initiation on treatment, and retention in care rates. This is accomplished in part by several hundred dedicated HIV testers and nurses who support ART initiation and management of opportunistic infections alongside MoHCC staff.
ZimPAAC also supports index testing through community linkages activities that help clients access HIV testing, especially sexual partners and biological children of existing HIV-positive clients who present to the health facilities. In an effort to improve index testing within MoHCC health facilities, ZimPAAC has implemented an assisted partner service model, known as Enhanced Index Case Testing. This program emphasizes reaching clients recently diagnosed with HIV and those whose blood tests show a high HIV viral load. Quality Improvement activities are a key part of ZimPAAC’s approach to improving outcomes for index testing. In 2019, a “change package” describing the interventions that have improved index testing was developed by ZimPAAC for national scale-up of the model.
ZimPAAC program activities also support retaining people living with HIV in care. Programs engage community linkage facilitators who work with facilities and communities to identify patients who have defaulted from treatment and return them to services.
In addition to HIV care and prevention for adults, ZimPAAC supports increased access to services for children and adolescents through Africaid’s community adolescent treatment supporters (CATS). CATS are HIV positive 18-to-24-year-olds trained to provide peer support, conduct demand-creation activities, build community engagement, and mobilize targeted HIV testing and outreach activities to bring services to this hard-to-reach group.
In addition to the first two objectives, ZimPAAC collaborates with MoHCC towards two additional objectives:
Strengthen and expand access to cervical cancer screening and treatment of precancerous cervical lesions among women living with HIV
Increase uptake of pre-exposure prophylaxis (PrEP) services through training, technical assistance and direct client support
Under the direction of PZAT, ZimPAAC also works closely with the MoHCC to support key-population-friendly programming in the public health sector facilities in Harare. PZAT supports health worker training at selected facilities and builds demand and knowledge of these services through community champions and engagement with vulnerable populations and advocacy and civil society organizations. PZAT also works to promote PrEP services for adolescent girls and young women in Mazowe district and among key populations in Harare.
The ZimPAAC consortium has supported high-quality health care worker (HCW) knowledge and skills in Zimbabwe with technologies such as applications with clinical resources for clinicians, tablet-based data collection, and self-study modules. Through the use of self-study courses, HCWs complete learning activities using case scenarios in either prevention of mother-to-child transmission client retention, HIV testing services for children and adolescents, or viral load testing. ZimPAAC also uses WhatsApp messaging groups as a training intervention during self-study for peer-to-peer learning and support. Tablet-based data collection has now become the norm for most sites.
ZimPAAC also continually works to strengthen its program monitoring systems, such as the deployment of TrainSMART as the national training database. Recently, ZimPAAC developed and introduced the ZimPAAC Data Improvement Plan (ZDIP)—a new system of electronic data collection tools that will improve reporting and give facility and district staff better access to data. The new digital forms in ZDIP offer built-in data quality checks, the ability to view graphs, and provides faster feedback to sites so they can use the data for facility-based improvements.
Since 2013, the ZAZIC Consortium has been implementing Voluntary Medical Male Circumcision (VMMC) as part of a combination HIV prevention package approved by the Ministry of Health and Child Care (MoHCC) in Zimbabwe. Unlike other VMMC programs in the region, the ZAZIC model uses an integrated approach, blending local clinic staff supported by MOHCC with partner staff. The ZAZIC consortium supports:
Training using MoHCC approved curricula, health workers in the supported districts are trained on the surgical technique as well as on demand creation
Development and implementation of age appropriate demand creation strategies
Support service delivery in 13 districts from consent procedures to post-surgical care and linkage to other services
Comprehensive monitoring and evaluation including continuous quality improvement and operations research
From 2013-2018, ZAZIC performed over 300,000 VMMCs with a reported moderate and severe adverse event rate of 0.3%. The safety, flexibility, and pace of scale-up associated with the integrated VMMC model appears similar to vertical delivery with potential benefits of capacity building, sustainability and health system strengthening. Although more complicated than traditional approaches to program implementation, attention should be given to this country-led approach for its potential to spur positive health system changes, including building local ownership, capacity, and infrastructure for future public health programming. Over 80% of the circumcisions occur in outreach settings, an approach that ensures wide coverage and expanded services in hard-to-reach locations.
Voluntary medical male circumcision (VMMC) is considered safe and the vast majority of men heal without complication. However, guidelines require multiple follow-up visits, which can burden staff and facilities with clients who are typically healing well. With funding from the National Institutes of Health (NIH), ZAZIC recently conducted a prospective randomized control trial (RCT) to determine if two-way texting (2wT) was as safe as routine post-operative visits and if it reduced workload in two high-volume VMMC sites near Harare, Zimbabwe.
Image of the 2wT App used to support the study.
Both clients and providers felt satisfied with the 2wT system and felt it could be ready for scale. Many clients reported feeling confident, comfortable, satisfied, and safe with text follow-up. Importantly, clients felt that 2wT saved them time and money. Providers also noted 2wT saved them time, empowered their clients to engage in the healing process, and addressed gaps in MC service quality.
It was recommended in the study that 2wT between providers and patients should be considered for future adaptation in other short-term care contexts. 2wT also appears far less expensive than active follow-up to improve patient safety: on average, post-VMMC follow-up under 2wT was $0.098 compared to $0.955 under routine care. 2wT was both less costly and more effective in identifying AEs relative to the expected rate of AEs. As such, I-TECH aims to scale 2wT in further testing among rural clients and guardians to improve patient care at lower cost.
The trial is registered on ClinicalTrials.gov, trial NCT03119337, and activated on April 18, 2017. https://clinicaltrials.gov/ct2/show/NCT03119337. This RCT was supported by the Fogarty International Center of the National Institutes of Health under Award Number R21TW010583.
Employing modern medical male circumcision within traditional settings may increase patient safety and further male circumcision scale up efforts in Sub-Saharan Africa. ZAZIC established a successful, culturally sensitive, partnership with the VaRemba, an ethnic group in Zimbabwe that practices traditional male circumcision. The VaRemba Camp Collaborative (VCC) was created to provide safe, standardized male circumcisions and reduce adverse events (AEs) during traditional male circumcisions. ZAZIC supported the VCC by providing key MC commodities and transport to help ensure patient safety. In 2017, the VaRemba granted permission to ZAZIC doctors to provide oversight of MC procedures and post-operative treatment for all moderate and severe AEs within the Camp setting. Of the Camp residents, 98% chose medical male circumcision.
The multi-year, iterative cycle of meetings and trust building ultimately resulted in the successful VCC, a model that may be replicable for others trying to combine modern male circumcision and traditional practice.
ZAZIC employs an innovative performance-based financing (PBF) system to speed progress towards ambitious voluntary medical male circumcision (VMMC) targets. The PBF schedule, which started at $25 USD and now varies from $6.50-$14 USD depending on the location and the circumcision team, is continually refined to set the program up for sustainable transition. The PBF is an incentive that is intended to encourage underpaid healthcare workers (HCWs) to remain in the public sector and to strengthen the public healthcare system. The majority of the incentive supports HCWs who perform VMMC alongside other routine services; a small portion supports province, district, and facility levels.
I-TECH conducted a qualitative study to assess the effect of the PBF on HCW motivation, satisfaction, and professional relationships. The study found that the PBF appreciably increased motivation among VMMC teams and helped improve facilities where VMMC services are provided. However, PBF appears to contribute to antagonism at the workplace and create divisiveness. To reduce workplace tension and improve the VMMC program, ZAZIC increased training of additional HCWs to share the PBF incentive more widely and strengthened integration of VMMC services into routine care.
Describing Adverse Events within VMMC Programs at Scale
I-TECH works diligently to review and revise procedures to identify, manage, and report adverse events (AEs). I-TECH’s previous publications on AEs reveal efforts to maintain high quality programming and emphasize patient safety alongside achievement of targets.
An evaluation published in the Journal of the International AIDS Society found that AEs were uncommon, with 0.3% of surgical and 1.2% of PrePex (a non-surgical VMMC device) clients experiencing a moderate or severe AE. However, the evaluation also found that younger clients were at greater risk of infection.
Increasing Understanding on the Timing and Type of AEs in Routine VMMC Programs at Scale
As VMMC expands in Sub-Saharan Africa, I-TECH works to ensure program quality matches efforts to increase program productivity. I-TECH ensures patient safety through patient follow-up to identify and treat AEs. The timing of routine follow-up visits in MC programs is designed to ensure patient safety by identifying, treating, and managing complications. Although routine follow-up timing may differ by country, in Zimbabwe, three follow-up visits are scheduled to ensure quality service provision and patient care: Visit 1 (Day 2); Visit 2 (Day 7); and, Visit 3 (Day 42).
I-TECH’s implementation science efforts use routine data collected from clients with AEs and has found that AEs followed distinct patterns over time. Using these findings, ZAZIC has been improving VMMC care by 1) improving counseling about MC complications following initial visits for clinicians, clients, and caregivers ; 2) distributing wound care pamphlets to clients and caregivers; and 3) emphasizing follow-up tracing for younger boys, ages 10-14, and their caregivers to provide additional targeted, post-operative counseling on AE prevention.
Increasing AE Ascertainment through Routine Quality Assurance Efforts
To further increase ascertainment of AEs, I-TECH recently conducted a quality improvement (QI) initiative to improve provider identification and reporting of AEs. ZAZIC Gold-Standard (GS) clinicians prospectively observed 100 post-MC follow-ups per site in tandem with facility-based MC providers to confirm and characterize AEs, providing mentoring in AE management when needed.
The QI data suggested that AEs may be higher and follow-up lower than reported and ZAZIC’s Quality Assurance Task Force is replicating this QA study in other sites; increasing training in AE identification, management, and documentation for clinical and data teams; and improving post-operative counseling for younger clients. Additional nurses and vehicles, especially in rural health clinics, are currently being trained and leveraged to further improve client follow-up and AE ascertainment.
Improving Data Quality
ZAZIC undertakes weekly, monthly, and quarterly data quality audits (DQA) to ensure data correctness and completeness. Intensive DQA processes were documented and availability and completeness of data collected before and after DQAs in several specific sites was assessed with the aim to determine the effect of this process on data quality. ZAZIC found that after the DQA, high record availability of over 98% was maintained and record availability increased. After the DQA, most sites improved significantly in data completeness and ZAZIC continues to emphasize data completeness to support high-quality program implementation and availability of reliable data for decision-making.
I-TECH builds local ownership and sustainability through collaborations throughout Zimbabwe. Under the CDC and PEPFAR awards, I-TECH has formed and leads two consortia – ZAZIC and ZimPAAC.
Voluntary medical male circumcision (VMMC) safely reduces the risk of female-to-male HIV transmission by up to 60%. Few men have any post-operative VMMC complication. However, current practice in Zimbabwe and throughout most of sub-Saharan Africa requires VMMC patients to return for multiple, in-person post-operative visits. With low complication rates, and severe healthcare worker shortages, these required visits are a burden for providers and patients — threatening achievement of critical HIV prevention targets. A two-way texting model studied by University of Washington researchers in Zimbabwe offers a new way to address this barrier by reducing provider workload while also safeguarding patient safety.
“These visits can be a barrier to male circumcision uptake and expansion in countries with severe health care worker shortages, as well as negatively impacting patients who needlessly pay for transport, miss work, and wait for unnecessary reviews,” said Principal Investigator Caryl Feldacker, PhD, MPH, at the International Training and Education Center for Health (I-TECH) in the University of Washington Department of Global Health.
The study included 721 VMMC patients in two locations in urban Zimbabwe. In the study, patients communicated directly with a health care worker through interactive text messaging for the critical 13 days post-VMMC, rather than returning for required in-person visits. By giving men the option to heal safely at home, or return to care when desired or if complications arose, the method dramatically reduced in-person visits by 85%. Texting also reduced follow-up costs by about one-third while improving the quality of care.
As compared to routine in-person care, the study yielded twice the number of reported complications. “This increased identification and reporting is a positive result that is likely attributable to improved counseling and men’s engagement in care. Through texting, men were empowered to observe their healing and report potential issues promptly, before they worsened,” said Feldacker.
Currently, most text-based health care efforts blast pre-defined messages to many people simultaneously, removing patients’ ability to communicate back with health care workers. In contrast, two-way texting between providers and patients provides interactive care, and the short time frame heightened participation: in the study, 93% of men responded to texts. Both providers and clients reported confidence in the texting option, feeling safe and highly recommending it for scale.
“With the current system, Zimbabwe could perform millions of unnecessary follow-up visits over the coming five years. The workload burden for health care workers and time lost for patients who are healing without complication is a significant burden for health care workers and clients alike,” said Feldacker. “Potential gains in efficiency and reduced costs through using two-way messaging are large.”
With funding from the U.S. Centers for Disease Control and Prevention (CDC), and in partnership with the Society for Family Health, the model will soon be tested in urban South Africa. The new, field-based research will further test two-way texting in a different geographical and patient context to better inform the model for adaptation and widespread scale-up.
Feldacker added that “while our findings are grounded in studies on male circumcision, our results are largely attributable to the methods rather than to a specific disease or condition.
“With minimal adaptation,” she continued, “two-way texting could streamline other post-operative care contexts or be re-configured for other similarly acute, episodic conditions where continuity of care within a short period is critical for patients, such as short-course TB treatment, post-operative healing, post-natal care or early childhood illnesses — diarrhea, pneumonia, malaria — laying the foundation for generalizing to other diseases and contexts.”
For more on the study, see the paper pre-published in the Journal of Acquired Immune Deficiency Syndromes (JAIDS):
The study was led by Caryl Feldacker, and co-investigators are Vernon Murenje (International Training and Education Center for Health (I-TECH), Harare, Zimbabwe); Mufuta Tshimanga (Zimbabwe Community Health Intervention Project (ZiCHIRE), Harare, Zimbabwe); Scott Barnhart, Isaac Holeman, and Joseph B. Babigumira (Department of Global Health, University of Washington); Sinokuthemba Xaba (Ministry of Health and Child Care, Harare, Zimbabwe); and technology partner Medic Mobile (Nairobi, Kenya).
The Zimbabwe 2wT study was supported by the Fogarty International Center of the National Institutes of Health under Award Number R21TW010583.