The Center for Stewardship in Medicine (CSiM) has joined the International Training and Education Center for Health (I-TECH) Network as a partner, operating within the University of Washington’s Department of Global Health. CSiM is a collaborative of over 80 rural hospitals across nine states in the U.S. working together on stewardship challenges through education, quality and process improvement, and mentoring.
I-TECH and CSiM will mutually benefit from collective decades of experience tackling rural health challenges – including workforce shortages, staff who wear “many hats,” and disparities in services – in the U.S. and around the world.
“CSiM is a collaborative of physicians, nurses, laboratory professionals, and pharmacists working to bridge bi-directional knowledge gaps between academic medical centers and rural health care facilities,” said John Lynch, MD, MPH, co-director of CSiM. “Like I-TECH, we value collaborative, anti-hierarchical work that honors expertise and experience at all levels of the health care system, and from all sectors.” Dr. Lynch leads the center with Chloe Bryson-Cahn, MD, and Zahra Kassamali-Escobar, PharmD.
The CSiM team with guest speakers at the center’s conference in Spokane, WA, May 2023. Photo courtesy of CSiM.
CSiM works in antimicrobial stewardship and infection prevention, building sustainable quality improvement programs, and providing customized, long-term technical assistance to rural health facilities. The center’s main activities include leading the UW Tele-Antimicrobial Stewardship (TASP ECHO®) project, a telementoring program; coordinating Intensive Quality Improvement Cohorts; and providing resources and tools to support facilities in reaching their goals and improving the quality of healthcare.
“I-TECH and CSiM share a dedication to finding innovative and local solutions to provide ongoing education and mentoring to health care workers in resource-limited settings,” said Pamela Kohler, BSN, PhD, I-TECH co-director. “We are incredibly excited about the opportunity to learn from each other.”
Currently, CSiM has projects in Arizona, Idaho, Illinois, Louisiana, Maine, Montana, Oregon, Utah, and Washington and is exploring opportunities to extend its model globally.
“CSiM’s inclusive, team-based approach results in work that really matters to communities in need – particularly those in underserved, hard-to-reach, rural areas,” said Ivonne Ximena “Chichi” Butler, MPH, I-TECH co-director. “This approach makes it a perfect fit within the I-TECH Network.”
The World Health Organization recommends countries routinely implement nationally representative HIV drug resistance (HIVDR) surveys among people infected with HIV to measure the level of drug resistance. The results of HIVDR surveys are a critical component of HIV programs and can guide changes to pediatric and adult antiretroviral therapy (ART) treatment regimens, including first- and second-line regimen decisions. I-TECH has been implementing HIVDR surveys in Malawi since 2016.
HIV DR Surveys Conducted Since 2016:
Infant HIVDR Survey: An HIVDR survey was conducted among infants aged 18 months and younger to determine the level of pediatric resistance to nonnucleoside reverse transcriptase inhibitors (NNRTI), nucleoside reverse transcriptase inhibitors (NRTI), and protease inhibitors (PI) ART drugs through exposure during pregnancy and breastfeeding. A total of 232 eligible remnant dried blood spot (DBS) samples from nine early infant diagnosis (EID)-approved laboratories were used for the diagnosis of HIV in infants between June 2016 and December 2017.
Antenatal Care (ANC)/Pregnant Women HIVDR Survey: An HIVDR survey was conducted to measure resistance to NNRTI, NRTI and PI drugs among ANC clients who were found to have a recent HIV infection. A total of 45 DBS samples from women with recent HIV infection were collected as part of the 2016 HIV sentinel surveillance survey and were successfully amplified and sequenced.
The next step in HIV surveillance activity is monitoring HIVDR among pregnant women initiating dolutegravir (DTG)-based regimens, as well as the potential emergence of DTG resistance in infants via mother-to-child transmission. A study of DTG resistance is currently underway in Malawi and will determine the level of DTG resistance in adults who are unable to achieve viral load suppression and DTG resistance in children < 15 years old who are unable to achieve viral load suppression.
Lydia Chwastiak
Lydia Chwastiak MD, MPH is a psychiatrist and internal medicine physician and Professor in the Department of Psychiatry and Behavioral Sciences and Adjunct Professor in Global Health in the University of Washington. Her research for the past 21 years has focused on improving the care and outcomes of people with chronic medical conditions and serious mental disorders. She has been a principal investigator (PI) or co-investigator on eight NIH-funded clinical trials of integrated care in both medical and community mental health settings, including MPI on the multi-center INDEPENDENT Study (R01 MH100390) which demonstrated the effectiveness of collaborative care for the treatment of depression among patients with poorly controlled type 2 diabetes in 4 diabetes centers in India.
At I-TECH, Dr. Chwastiak is also the PI on a large global HRSA-funded grant to support capacity building for sustainable HIV services in Jamaica, Trinidad and Tobago, India, Mozambique, and Ukraine (U91HA06801). The goal of Capacity Building Program is to improve health outcomes for people living with HIV (PLHIV) along the HIV care continuum by building sustainable health systems. The program seeks to improve the efficiency and client-centeredness of HIV care systems by strengthening the operational and adaptive capacities of health institutions and the health workforce; expand the use of evidence-based methodologies and best practice approaches to improve health outcomes for PLHIV; increase the functionality and coverage of innovative technology platforms to improve HIV service delivery, public health communication, and data use for decision making; and strengthen equitable collaborations between country governments, implementing partners and communities to achieve and sustain epidemic control.
In addition to her work with I-TECH, Dr. Chwastiak is Associate Director of the UW Behavioral Research Center in HIV (BIRCH), an NIMH-funded developmental AIDS Research Center and directs the Center’s Integrated Care Research Core. She also is the PI and co-director of the SAMHSA-funded Northwest Mental Health Technology Transfer Center (Northwest-MHTTC), which provides training and technical assistance to support the behavioral health workforce of HHS Region 10 (AK, ID, OR and WA) to disseminate and implement evidence-based practices for mental disorders.
The 2023 IAS Conference on HIV Science logo. Read the full background and inspiration behind the 2023 IAS Logo. Image credit: IAS
The International AIDS Society (IAS) hosted the 12th IAS Conference on HIV Science on 23 – 26 July 2023 in Brisbane, Australia, and virtually. This biennial conference brings together top HIV researchers, experts, and scientists for presentations and discussions on the latest advances in HIV research and practice.
This year, representatives from the International Training and Education Center for Health (I-TECH), I-TECH’s partner network organizations, and the Centers for Disease Control and Prevention (CDC) shared findings from I-TECH-supported programs in India, Malawi, and Zimbabwe. Read the ePoster abstracts below.
Voluntary medical male circumcision (VMMC) decreases the risk of female-to-male HIV transmission by about 60%.[1] I-TECH Network partner the Zimbabwe Technical Assistance, Training, and Education Center for Health (Zim-TTECH) supports innovative VMMC engagement solutions that are tailored to the populations they serve.
Caravans Allow for Mobile Services and Door-to-Door Outreach
VMMC Mobilizers engage with men at a farm compound in Goromonzi District. Photo credit: Zim-TTECH
Makumbe Hospital in Goromonzi District, Zimbabwe, serves a population of more than 100,000 people, including the rapidly expanding population of surrounding townships. Zim-TTECH-led consortium ZAZIC has run the Makumbe Hospital site since October 2018 and supports the VMMC team there.
This population within the hospital’s catchment area primarily comprises informal traders selling necessities such as groceries, garden produce, or second-hand clothes, while others run at-home small businesses that manufacture furniture, iron and steel products, and other wares.
“It’s difficult for economically active young men to leave their businesses and attend to VMMC at a venue away from their premises or market,” said Lewis Masimba, VMMC Program Manager at Zim-TTECH.
In light of this challenge, the team implemented a mobile caravan, which could increase the number of men receiving circumcisions by taking services out of the medical facility and bringing them closer to the concentrated settlements of Domboshava Showground, Mungate, and Mverechena townships and nearby farm compounds.
The caravan has been in use in the district since January 2023, and it has vastly shortening the period between client engagement and service delivery. In most cases, two mobilizers at a time will engage with potential clients within the townships, while another three will conduct intensive door-to-door visits in residential areas.
Mobilization efforts include one-on-one and small group discussions at market stalls, small businesses, and drinking spots, where mobilizers will answer questions and distribute information about VMMC. Sometimes the caravan is supported by a roadshow van and dancers who disseminate VMMC information through edutainment.
“The caravans have so many advantages,” said Mr. Masimba. “Men are able to access the VMMC services near their workplaces, minimizing disruptions to their daily routines. The caravan has also brought convenience and privacy to those who did not feel comfortable being ferried in program vehicles to and from the hospital.”
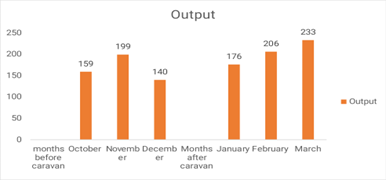
Fig 1: Outputs three months before receiving the caravan and three months after receiving the caravan
Since the site started utilizing the caravan, the number of men who have received VMMC each month has increased from 159 to 233 (Fig. 1).
On the heels of this success, the ZAZIC teams will continue exploring other combination approaches involving engagement activities such as pool/snooker, soccer, and music roadshows to reach hard-to-convince men in their localities.
Peer-to-Peer Learning Takes Center Stage in Performing Arts Program for Adolescents
Eight secondary schools enrolled in the drama competition. Photo credit: Zim-TTECH
The performing arts have been used since time immemorial as motivators to rally communities toward common goals, to relieve stress, and as an effective teaching tool across diverse cultures and religious settings. They are a particularly effective method for engaging adolescents both in and out of schools. As teens seek independence from their parents, the influence of peers becomes increasingly important, and performing arts are a fantastic way to employ peer-to-peer learning strategies.
Harnessing these strategies, ZAZIC uses drama in several districts to complement efforts already made by VMMC teams and teachers who have previously used sporting events and lectures to communicate with students.
In a particularly successful case, Hurungwe District chose to use a drama competition to communicate VMMC and other health messages to adolescents. The goals of the competition included effective peer-to-peer learning, outreach to a large audience, and the demystification of VMMC.
Roadshows to promote the competition were held at major townships to create awareness of the event and invite members of the public to attend. Eight secondary schools enrolled in the competition, and teams of adolescents led the process of writing and directing short, 30-minute performances incorporating messages in a provided guide.
The guide emphasized use of appropriate language, the need to double-check facts; and encouragement of uptake of VMMC and related services, such as HIV testing and counseling and cervical cancer screening.
More than 1,000 people attended, including students, parents, and staff from all competing schools.
“Matawu Secondary School ultimately won the drama competition, but all of the schools did a wonderful job explaining VMMC and its benefits,” said Mr. Masimba. “Messaging also emphasized abstinence for adolescents, the importance of the HPV vaccine for girls, and details about the VMMC procedure. The level of accuracy of information was extremely high.”
Importantly, two of the performances highlighted communities that reject medical interventions and stressed the need for participation by all.
A total of 182 VMMCs were attained by adolescents aged 15 to 19 years old immediately after the competition. Those who were not ready were booked for the procedure and will be followed up with by school health masters and community mobilizers.
John Lynch, MD, MPH is an infectious diseases physician focused on improving the operations and capacities of healthcare teams to improve patient care and safety. He is an Associate Medical Director at Harborview Medical Center (HMC), a mission-driven, Level-1 burn and trauma teaching hospital that is part of the University of Washington (UW) School of Medicine. At HMC, he leads the hospital’s Infection Prevention & Control (IPC), Employee Health, and Sepsis Programs, and was the lead clinician for UW Medicine’s COVID-19 emergency response. Dr. Lynch is also a Professor of Medicine in the Division of Allergy & Infectious Diseases in the University of UW Department of Medicine.
Dr. Lynch co-leads the Center for Stewardship in Medicine (CSiM), a group of physicians and pharmacists working to bridge knowledge gaps (in both directions) between academic medical centers and rural health care facilities. Their work is mainly in antimicrobial stewardship and infection prevention but also extends to building quality improvement programs in those facilities. CSiM is composed of three main activities, including UW Tele-Antimicrobial Stewardship, a telementoring program, the Intensive Quality Improvement Cohorts, and resource/tool development to support the goals of the program.
In addition, Dr Lynch also works with Dr. Peter Rabinowitz (PI) to provide subject matter expertise on a long-running project to build IPC capacity in hospitals in Kenya as part of the I-TECH Global Health Security Agendaproject.
Population movement, limited public health infrastructure, different country reporting systems, and poor environmental conditions increase incidence of certain infectious diseases across borders. Communities living in border areas are at increased vulnerability for and worse outcomes from infectious diseases such as COVID-19 and other priority pathogens.
The Integrated Next-generation Surveillance in Global Health: Translation to Action (INSIGHT to Action) project is a five-year cooperative agreement with the US Centers for Disease Control and Prevention to assess and strengthen global public health surveillance systems using a One Health approach. The INSIGHT project leverages the capacity building strengths of I-TECH and the One Health disease surveillance expertise of the Center for One Health Research, with a model of engaging local institutions and experts in countries where it will be working in a shared partnership model.
In its first year, the INSIGHT project focused on an in depth assessment of the public health surveillance systems in Peru, in partnership with experts from University of Peru Cayetano Heredia. The completed assessment has now catalyzed the formation of a technical working group with representation across multiple government agencies that will work with other stakeholders including the World Bank at implementing measures to strengthen regional and country capacity to detect, respond to, control, and prevent emerging disease threats to health security.
The INSIGHT surveillance work in Latin America is also now expanding to involve Paraguay, Brazil, Argentina, and Colombia.
IDASH TRAINING PROGRAM
In 2023, the INSIGHT program launched the Informatics and Data Science for Health (IDASH) training program in Eastern Europe and Central Asia. The goals of IDASH are to enhance capacity to create and use public health information systems that enable the capture, management, analysis, dissemination, and use of reliable, timely information to improve population-level health outcomes, as well as strengthen regional capacity to effectively respond to future global health challenges.
UKRAINE RECOVERY
Building on lessons learned from the Peru assessment work, the INSIGHT team is now working with the Ukraine Public Health Center on expanding sentinel and event based surveillance systems in Ukraine and strengthening the capacity of the public health system for emergency management of chemical biological, radiological, and nuclear threats. The INSIGHT team has organized a workshop in Poland bringing together key principals from the Ukraine ministry of health and local health departments to accelerate the pace of activities in support of public health in the country. INSIGHT is coordinating technical working groups on Early Warning and Response, Public Health Emergency Management, and Surveillance strengthening.
Public Health Surveillance
I-TECH works in collaboration with key stakeholders, including communities, government entities, and the Centers for Disease Control and Prevention (CDC), to strengthen and implement surveillance programs focused on emerging disease threats, HIV recent infection, birth defects surveillance, and hospital acquired infections in sub-Saharan Africa. Eastern Europe, Asia, and South America.
In Malawi, I-TECH has supported the implementation of an active hospital-based birth surveillance system at four high-volume facilities in Malawi since 2016, and beginning in 2019, I-TECH began implementing recent HIV infection surveillance in April 2019.
In 2022, as part of the Integrated Next-generation Surveillance in Global Health: Translation to Action (INSIGHT to Action) project, I-TECH, the Peruvian Ministry of Health, the Universidad Peruana Cayetano Heredia, and CDC collaborated on a situational analysis to assess areas for potential strengthening of the Peruvian disease surveillance systems. In 2023, the INSIGHT for Action project launched the Triple Border Disease Surveillance Strengthening Program.
In Kenya, the I-TECH Kenya office is working with CDC on implementing surveillance for hospital acquired infections (HAI) in low resource settings, with a focus on surgical site infection surveillance.
Migrating waterfowl from Asia, Africa, and Europe intersect in Georgia, which increases the potential for novel avian-origin influenzas to emerge ... Read More
The Integrated Next-generation Surveillance in Global Health: Translation to Action (INSIGHT to Action) project is a five-year cooperative agreement with the ... Read More
Despite establishing COVID-19 monitoring measures within the existing routine national surveillance system and significant efforts to conduct testing, contact tracing, ... Read More
Population movement, limited public health infrastructure, different country reporting systems, and poor environmental conditions increase incidence of certain infectious diseases ... Read More
The World Health Organization recommends countries routinely implement nationally representative HIV drug resistance (HIVDR) surveys among people infected with HIV ... Read More
I-TECH Kenya’s Global Health Security Agenda (GHSA)-funded programs aim to advance the GHSA goals of preventing , detecting, and responding ... Read More
The Frontline Field Epidemiology Training Program (Frontline FETP) enhances the capacity of HIV and AIDS surveillance and strengthens health systems ... Read More
In collaboration with the Malawi Ministry of Health (MOH) and Centers for the Disease Control and Prevention (CDC), I-TECH has ... Read More
One Health
Human disruptions to natural systems are causing climate change and other major environmental upheavals including biodiversity loss, zoonotic disease emergence, toxic pollution, heat emergencies, and flooding that will have major impacts on the health of human and animal populations. To reflect the intersectionality and interconnectedness of the health of humans, animals, and the shared (and rapidly changing) environment, I-TECH partners with the Center for One Health Research in designing and implementing programs that use the One Health approach to prevent, detect, and respond to emerging disease threats. I-TECH’s One Health approach focuses on strengthening disease surveillance systems and laboratories to detect and assess new infectious disease threats, as well as detecting “sentinel” cases of disease in humans and animals that are indicators of health impacts of environmental change.
In 2022, I-TECH formed the Global One Health Group to support the prevention, detection, and response to emerging disease threats throughout the world. By leveraging the strength and expertise of the University of Washington Center for One Health Research and other UW partners, I-TECH is providing effective training, technical assistance, and laboratory services to support capacity and systems strengthening in affected communities. The Global One Health Group includes experts in zoonotic and other infectious diseases, antimicrobial resistance, public health, animal health, environmental health, and implementation science.
The Integrated Next-generation Surveillance in Global Health: Translation to Action (INSIGHT to Action) project is a five-year cooperative agreement with the ... Read More
 The Center for Stewardship in Medicine (CSiM) has joined the International Training and Education Center for Health (I-TECH) Network as a partner, operating within the University of Washington’s Department of Global Health. CSiM is a collaborative of over 80 rural hospitals across nine states in the U.S. working together on stewardship challenges through education, quality and process improvement, and mentoring.
The Center for Stewardship in Medicine (CSiM) has joined the International Training and Education Center for Health (I-TECH) Network as a partner, operating within the University of Washington’s Department of Global Health. CSiM is a collaborative of over 80 rural hospitals across nine states in the U.S. working together on stewardship challenges through education, quality and process improvement, and mentoring.