The International AIDS Society (IAS) virtually hosted their 23rd International AIDS conference (AIDS 2020: Virtual) on 6-10 July 2020. The AIDS 2020: Virtual theme was resilience, to celebrate and acknowledge the strength of the HIV community and the significant advances in treatment, while also addressing gaps in treatment, prevention, and care.
Representatives from the International Training and Education Center for Health (I-TECH) virtually presented the following posters with accompanying audio recordings:
- Fred Bangara, MLT, BTech, MSc, I-TECH Malawi Laboratory Specialist, presented an e-poster that looked at the feasibility of implementing point-of-care rapid testing for recent infections in routine HIV testing service settings titled, “Comparison of POC RTRI results with laboratory-based LAg avidity and viral load test results.”
- Laura Muzingwani MBChB, PGDPH, I-TECH Namibia Cervical Cancer Prevention Lead Physician, presented an e-poster that analyzed data about HIV positive patients’ first cervical cancer screening and the severity of cervical lesions titled, “Patient age and cervical lesion severity by HIV-status: The first 13 months of VIA and cryotherapy/thermocoagulation implementation in Namibia.”
- Malango Msukwa, BSc, MPHc, I-TECH Malawi Monitoring, Evaluation, and Data Manager, received a scholarship from IAS to attend AIDS 2020: Virtual and presented a late-breaker e-poster on a study that evaluated the uptake of a new HIV surveillance system and described which populations have continued HIV transmission titled, “Characterizing recent infections among persons with new HIV-1 diagnoses in Malawi.”
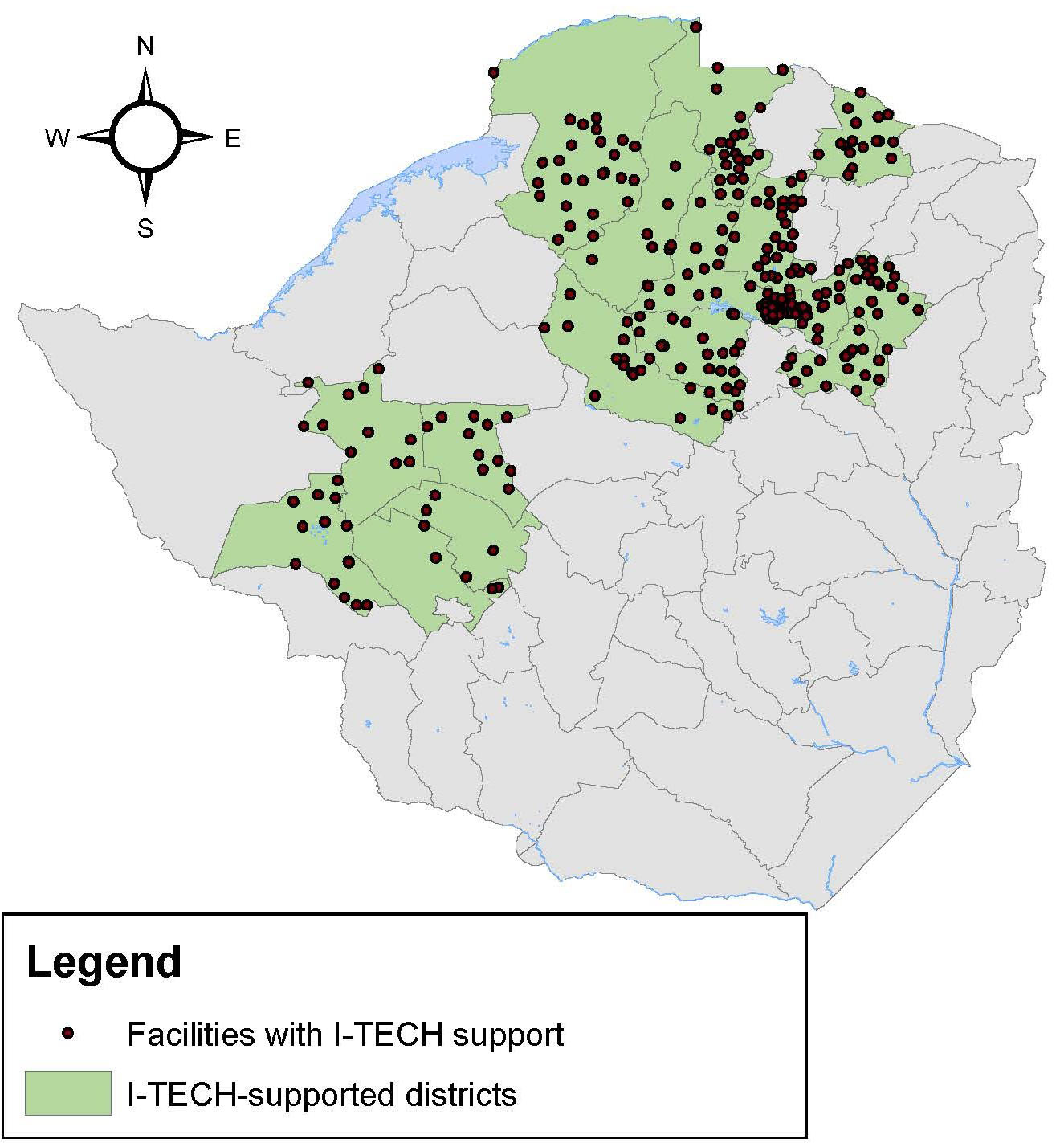
- Vernon Murenje, MBcHB, MSc, VMMC Program Manager for the Zimbabwe Technical Assistance Training and Education Center for Health (Zim-TTECH), presented an e-poster exploring how program quality is impacted by increased and ambitious targets titled, “Balancing priorities: quantity versus quality within a voluntary medical male circumcision program operating at scale in Zimbabwe.”
In addition to the I-TECH representatives presenting their posters, representatives from the Centers for Disease Control and Prevention (CDC) and Health Alliance International (HAI) also presented data from I-TECH programs in Malawi and Mozambique.
- Melissa Arons, MSc, from the CDC presented data from the I-TECH Malawi recency surveillance program in an e-poster titled, “HIV recent infection surveillance: Healthcare worker acceptability and feasibility of integrating the rapid test for recent infection into HIV testing services in Malawi, 2019.”
- Wilson Hammet, MPH, presented data about scaling up HAI’s mental health intervention under I-TECH’s multi-country cooperative agreement funded by HRSA, the International AIDS Education and Training Center, during an oral abstract session titled, “Scaling up a lay counselor-delivered transdiagnostic mental health intervention (CETA) to improve the HIV care cascade in Sofala, Mozambique.”